
Every hospital that offers a trial of labor knows this can happen. The American College of Obstetricians and Gynecologists is clear that a trial of labor should be attempted only in a setting where an emergency cesarean can be performed. The risk is foreseeable. Because it is foreseeable, the law expects a hospital to be ready for it. Being unprepared for a known emergency is not bad luck. It is a failure of planning.
A uterine rupture during labor is measured in minutes. From the first warning sign to the safe delivery of the baby, a hospital has only a short window to act. When the team uses that window efficiently and doesn’t waste time, the baby can be born healthy. When the team is slow, distracted, or unprepared, those same minutes become the difference between a healthy child versus a lifelong injury or even death.
If your delivery turned into an emergency uterine rupture and your family was harmed, you may have been told the rupture itself caused everything. That is only part of the story. This article explains the response a hospital owes you when a rupture happens, and how a slow response can turn a survivable event into a tragedy.
The clock starts at the first warning sign
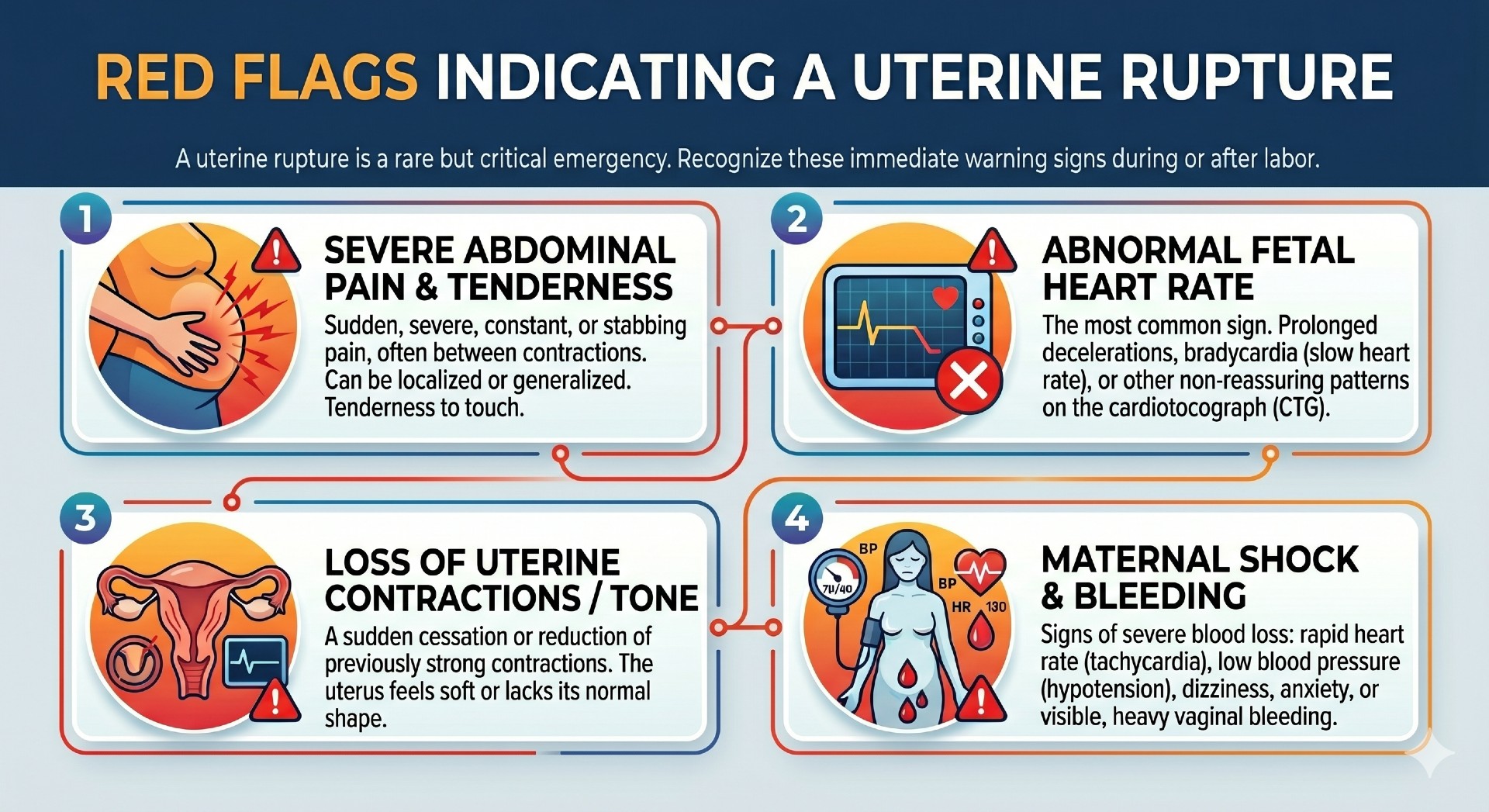
A rupture rarely arrives without notice. The most common early sign is a sudden, severe drop in the baby’s heart rate. Other signs include new abdominal pain, pain breaking through an epidural, unexpected vaginal bleeding, a falling maternal blood pressure, and the baby’s head sliding back up the birth canal.
When these signs appear, the response clock starts. A trained team should not wait for proof. It should treat a suspected rupture as a rupture and move at once. Every minute the baby’s oxygen supply is interrupted, the risk of permanent brain injury grows.
What a fast, competent response looks like
Once a rupture is suspected, a well-run labor unit moves through a clear sequence without delay. A surgeon and anesthesia provider are called and arrive quickly. An operating room is readied. The mother is moved. The baby is delivered, almost always by emergency cesarean section. A team stands ready to resuscitate the newborn and to control the mother’s bleeding.
Hospitals often plan around a benchmark of being able to begin an emergency cesarean within about thirty minutes of the decision. But a benchmark is a floor, not a goal. In a true rupture, faster is better. The standard is not whether the hospital hit a number. It is whether the team moved as quickly as a careful, well-prepared team should have.
Where the response breaks down
In our review of birth injury cases, the same delays appear again and again. Each one steals minutes a baby cannot spare.
- No one was watching the fetal monitor, so the first warning sign was noticed late.
- A nurse saw the warning sign but did not escalate it to a physician quickly enough.
- The physician was not in the hospital and had to travel in.
- No anesthesia provider was immediately available.
- No operating room was open and ready.
- The team treated the warning signs as a problem to keep watching rather than an emergency to act on.
Any one of these gaps can stretch a delivery past the point where the baby can be saved from harm. Stack two or three together, and a survivable rupture becomes a catastrophic injury.
Why the timeline is the heart of the case
A birth injury case involving a rupture is, at its core, a study of time. The medical record contains a detailed timeline. The fetal monitor strips are time-stamped. Nursing notes record when signs appeared and when calls were made. Orders, anesthesia records, and operating room logs all carry times.
By laying these records side by side, it becomes possible to reconstruct the emergency minute by minute. What did the hospital do to prepare and be ready for a uterine rupture? When did the heart rate drop? When was a doctor told? When was the decision to operate made? When was the baby actually born? The gaps between those moments tell the story. When the gaps are too long, and a healthy baby was harmed inside them, that is where responsibility lies.