
You went into the hospital expecting to bring your baby home. You had been told a vaginal birth after your cesarean was a reasonable choice. Then something went wrong. Maybe your baby’s heart rate dropped and would not recover. Maybe you felt a sudden, tearing pain. Maybe the room filled with people and no one would tell you what was happening. Now you are reading this because the answers you have been given do not add up.
What a uterine rupture is
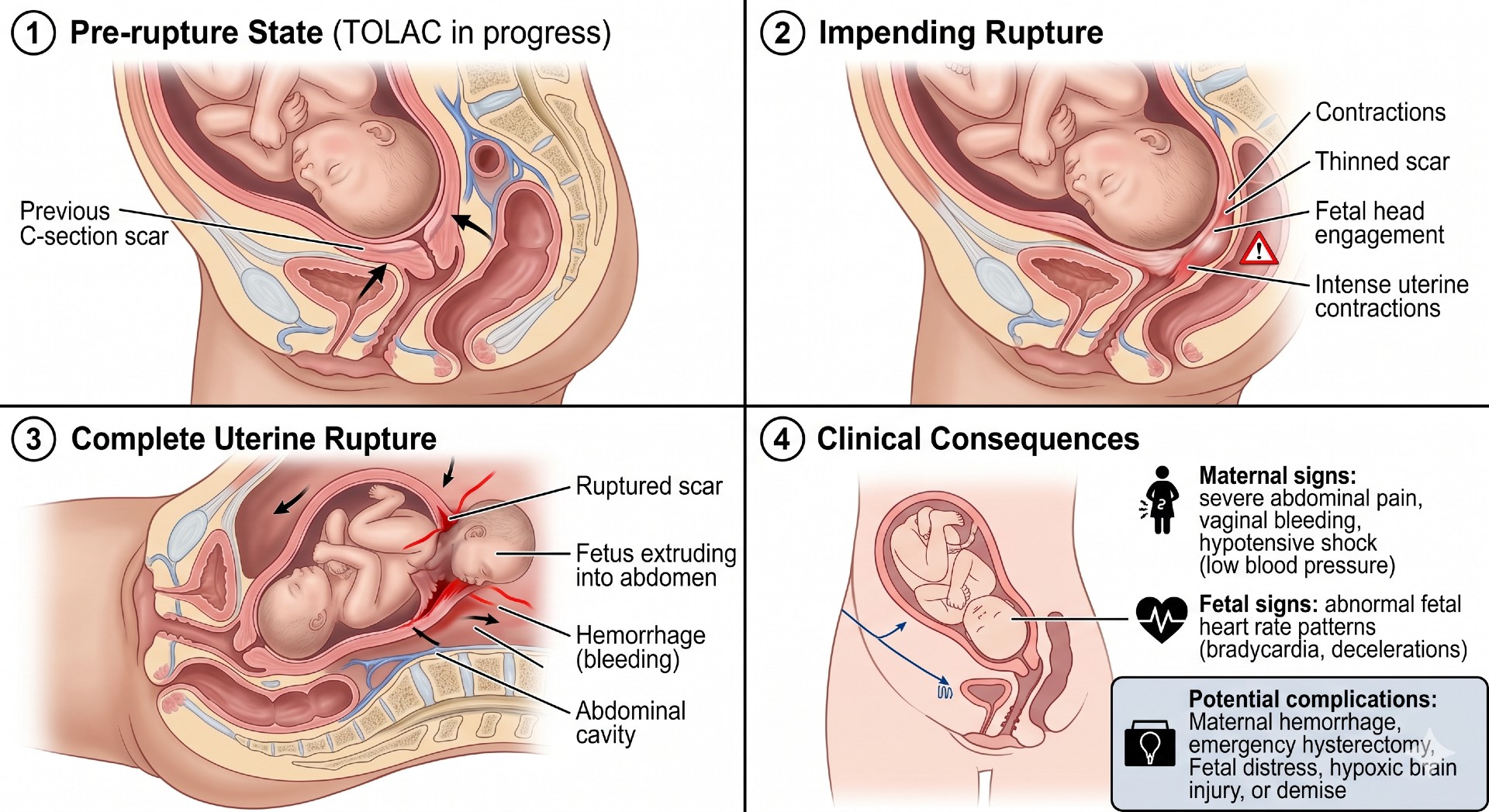
When a woman has a baby by cesarean, the surgeon cuts through the wall of the uterus. That cut heals into a scar. The scar is strong, but it is not as strong as the original muscle.
During a later labor, the uterus contracts hard, over and over, for hours. In a small number of women, the old scar gives way. The uterine wall tears open. This is a uterine rupture. It is a true emergency.
When the uterus tears, the baby can lose its oxygen supply within minutes. The placenta may separate. The baby can be pushed partly or fully out of the uterus and into the mother’s abdomen. The mother can bleed heavily. Both lives are at risk at the same time.
How often it happens
Uterine rupture is uncommon. That is one reason a trial of labor after cesarean, often called TOLAC, is offered at all. For a woman with one prior low-transverse cesarean, the American College of Obstetricians and Gynecologists (ACOG) places the risk of rupture during a trial of labor at roughly 0.5 to 0.9 percent.
A number under one percent sounds small. But two things matter here. First, the risk is not zero, and every hospital that offers TOLAC knows it. Second, a rare event is still a foreseeable one. When something is known to happen, the standard of care requires a plan for it.
The warning signs doctors are trained to catch
A uterine rupture rarely happens without warning. In most cases the body sends signals first. The medical literature and ACOG’s own guidance describe a cluster of signs that should put a labor and delivery team on high alert.
The most common and most important sign is a change in the baby’s heart rate. A sudden drop in the fetal heart rate, called bradycardia, is the single most frequent finding before a diagnosed rupture. ACOG identifies the fetal heart tracing as the most reliable early clue.
Other signs a team should never ignore include:
- New or severe abdominal pain, sometimes felt between contractions
- Pain that breaks through a working epidural
- Vaginal bleeding that is not expected
- A drop in the mother’s blood pressure or a rising heart rate
- Loss of fetal station, meaning the baby’s head moves back up the birth canal instead of down
- A change in the shape of the contraction pattern or a sudden stop in labor progress
No single sign proves a rupture by itself. That is the point. A trained team is supposed to read these signs together and act before the picture is complete.
What the standard of care requires
A trial of labor after cesarean is not an ordinary labor. ACOG is direct about this. A TOLAC should be attempted only where the staff and equipment for an emergency cesarean are available, and the mother needs continuous electronic fetal monitoring throughout.
Continuous monitoring exists for one reason. It is the early warning system. If the monitor is removed, if the signal is lost for long stretches, or if no one is watching the strip, the warning is missed. When the warning is missed, the response comes too late.
Once a rupture is suspected, the plan is simple to state and hard to do well. The baby must be delivered immediately, almost always by emergency cesarean. The mother’s bleeding must be controlled. Every minute counts, because the injury to the baby grows with every minute the oxygen supply is cut off.
Where care goes wrong
In our work on birth injury cases, certain failures appear again and again. A rupture itself is not always negligence. But the response to it often is.
We look closely at whether the team recognized the warning signs. We look at whether the fetal monitor was used correctly and read by someone qualified. We look at how long it took to move from the first sign of trouble to the actual delivery of the baby. We look at whether the hospital had the anesthesia and surgical staff on hand that a trial of labor demands. And we look at whether the mother should ever have been offered a trial of labor in the first place.
When a strong, healthy baby suffers a brain injury during a trial of labor, the cause is rarely bad luck alone. It is often a warning that was on the screen and a response that came too slowly.