
This article explains how doctors are supposed to decide who is a good candidate for a trial of labor after cesarean. It explains who should not be offered one at all. And it explains what it means when a doctor steers a woman toward a delivery plan that was wrong for her.
A trial of labor is a choice that must be matched to the patient
A trial of labor after cesarean, often called TOLAC, is an attempt to deliver vaginally after a prior C-section. A successful trial ends in a vaginal birth after cesarean, or VBAC.
For many women, a trial of labor is a reasonable and safe option. The American College of Obstetricians and Gynecologists supports it for appropriate candidates. But that last phrase carries all the weight. A trial of labor is not safe for everyone. The job of the doctor is to sort out who is a good candidate and who is not. When that sorting is done carelessly, a woman can be placed at a risk she never should have faced.
Who is generally a good candidate
ACOG describes the typical good candidate in clear terms. Most women with one prior cesarean delivery through a low-transverse incision are candidates for a trial of labor and should be counseled about it and offered the option.
A low-transverse incision is a side-to-side cut across the lower part of the uterus. It is the most common type, and it is the type least likely to tear in a later labor. Other factors improve the odds of a safe and successful trial. They include a prior vaginal delivery, a labor that begins on its own, and a reason for the first cesarean that is not likely to repeat.
Who should not be offered a trial of labor
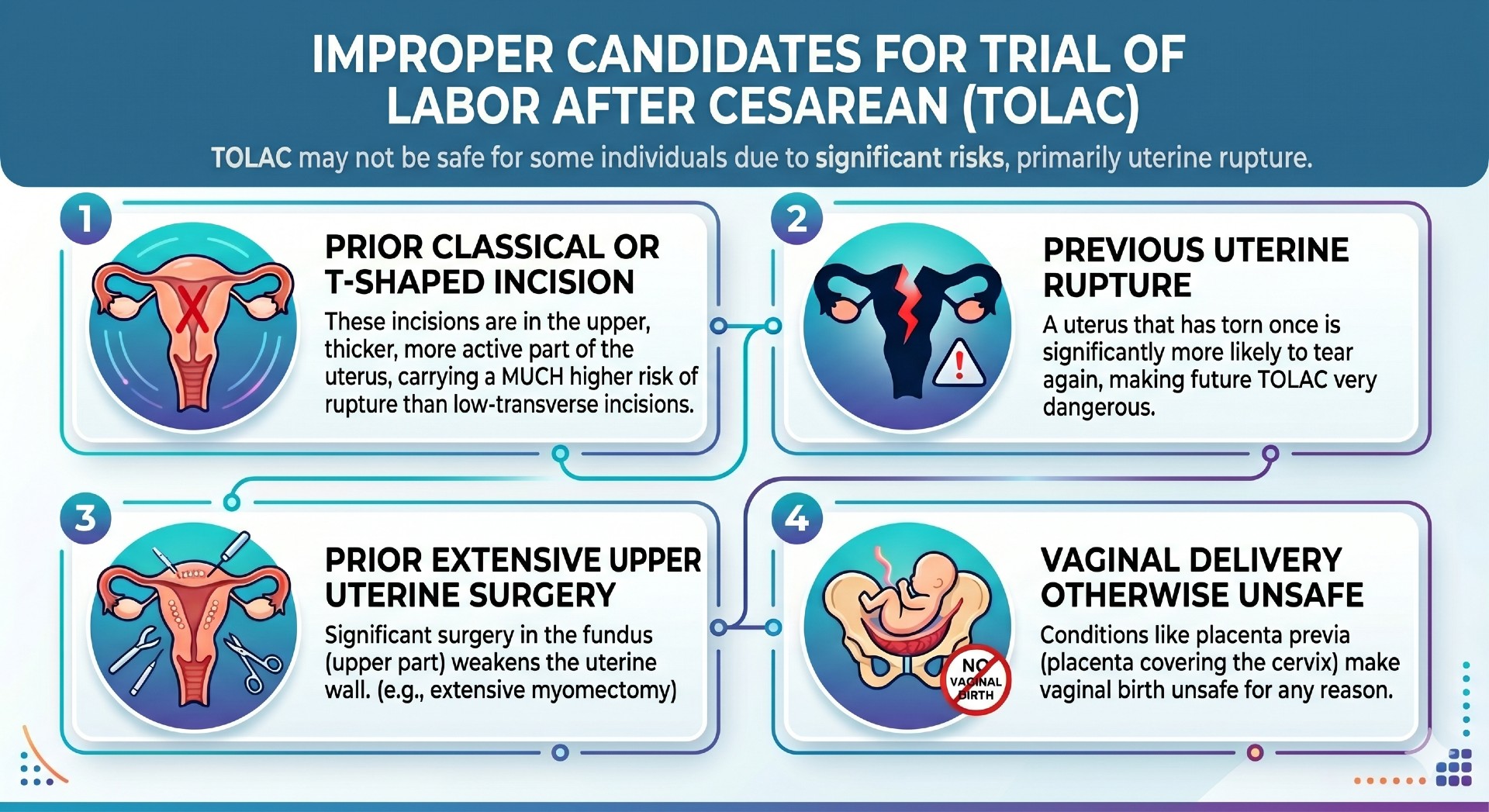
This is where careful patient selection matters most. ACOG identifies women who are at high risk of uterine rupture and who are generally not candidates for a planned trial of labor. They include:
- Women with a prior classical or T-shaped uterine incision, rather than a low-transverse one. These incisions involve the upper, thicker, more active part of the uterus and carry a much higher risk of rupture.
- Women who have had a prior uterine rupture. A uterus that has torn once is far more likely to tear again.
- Women with prior extensive surgery on the upper part of the uterus.
- Women for whom a vaginal delivery is unsafe for another reason, such as a placenta that covers the cervix.
For these women, a trial of labor is not a balanced choice between two reasonable paths. It is an exposure to a serious and foreseeable danger. The standard of care is to identify these patients and recommend a planned repeat cesarean instead.
The type of incision is not the same as the type of skin scar
Many women carry a low, horizontal scar on their skin and assume the cut on the uterus matched it. That is not always true. The skin scar and the uterine incision are separate. A surgeon can make a low skin incision and still cut the uterus differently if the situation demands it.
This is why the records from the first cesarean matter so much. The operative report from that first delivery describes exactly how the uterus was cut. A doctor counseling a woman about a trial of labor is expected to know what that report says. Assuming a low-transverse incision without checking is a shortcut that can have severe consequences.
Counseling is part of candidate selection
Selecting the right candidate is not only about a yes-or-no decision. It is also about an honest conversation. ACOG stresses shared decision making. A woman is supposed to be told her individual likelihood of a successful vaginal birth and her individual risk of uterine rupture. That conversation, and the decision that follows, should be documented.
A woman cannot give true consent to a trial of labor if she was never told the real risks, or if she was pushed toward one path without an honest discussion of the other. When the counseling is incomplete or one-sided, the choice was never really hers.
Where care goes wrong
In cases involving a trial of labor, improper patient selection is one of the failures we look for first. At Lupetin & Unatin, we review the operative report from the prior cesarean to see how the uterus was actually cut. We look at whether the doctor accounted for a prior rupture or prior uterine surgery. We look at whether the woman was told her real, individual risk, or only a reassuring summary. And we look at whether a planned repeat cesarean should have been recommended instead.
When a woman who was never a safe candidate is guided into a trial of labor and a rupture follows, the injury did not begin in the delivery room. It began with a decision made weeks earlier.