She Went to the Emergency Room Three Times.
They Sent Her Home Every Time. She Died at 28.
A young woman’s severe headache was dismissed as a migraine. Twice. By the same emergency room doctor. The blood clot in her brain was never diagnosed. One month after her wedding, her family was planning her funeral.
They were supposed to be starting their life together. Sarah and Matt got married in September in her parents’ backyard, the same yard where she grew up, where the family held every holiday and birthday for as long as anyone could remember. She was 28. She’d just finished law school. She was about to start a new job as a youth counselor, and she and Matt had been talking about having kids.
A month later she was gone.
An emergency room doctor saw her three times over two days for the worst headache of her life. He never ordered the imaging that would have shown a massive blood clot in her brain. He gave her the same sedating medication cocktail on each visit, watched her symptoms temporarily improve, and sent her home. By the time a different doctor finally ordered advanced imaging on the third visit, it was too late. She seized, her brain bled, and she was pronounced dead that night.
Lupetin & Unatin represented Sarah’s family. The case resolved with a multi-million dollar settlement.
“Multiple Red Flag Symptoms”
It started on a Monday morning. Sarah woke up with a stabbing headache, the kind she’d never had before in her life. Nausea. Vomiting. Dizziness. Changes in her peripheral vision. Tylenol didn’t touch it. By the afternoon she went to an urgent care clinic.
The physician assistant at the urgent care took one look at this picture and did exactly what she was supposed to do. A 28-year-old woman with no headache history, presenting with a sudden severe headache, vomiting, vision changes, and a heart rate in the 40s. That is a textbook red-flag presentation. The PA documented “multiple red flag symptoms that likely warrant imaging” and told Sarah to go straight to the hospital emergency department. She didn’t try to treat it herself. She recognized it was above her level of care. She sent Sarah where she needed to go.
Sarah and her mother, Linda, drove to one hospital but left after sitting in the waiting room for hours without being seen. They called a friend who worked security at another hospital nearby and were told the ER was basically empty. So they went there instead.
Sarah walked through those doors at about 11:00 p.m.
The First Visit to the Emergency Room
The ER doctor, Dr. Hayward, evaluated her. Sarah told him she’d woken up with a headache she’d rate a 9 out of 10. She was dizzy, nauseated, vomiting. She had never had a headache like this before. Never had migraines.
Dr. Hayward ordered a CT scan of her head without contrast. It came back clean. No acute bleeding. He ran bloodwork and tested for a urinary tract infection. Then he gave her what’s called a “migraine cocktail,” a combination of IV medications including Reglan, Benadryl, and Antivert. The cocktail is designed to knock out headache symptoms and sedate the patient. And it worked, at least temporarily. Sarah felt better and her headache eased.
So he sent her home.
He never ordered an MRI. Never ordered a CT with contrast or a CT venogram. Never did a lumbar puncture. He didn’t record anything about the fact that Sarah had received the Johnson & Johnson COVID vaccine about two weeks earlier. He documented almost nothing about her medical history. He treated the pain and moved on.
Sarah was discharged at 2:41 a.m. with diagnoses of non-intractable headache, dizziness, and UTI.
The Second Visit to the Emergency Room
The headache never stopped. Less than 17 hours later Sarah was back in the same ER. Dr. Hayward was working again. He recognized her. His patient from last night, back again, still hurting. And now she had a new symptom. Blurred vision.
Think about what that means from a medical standpoint. You have a young woman with no headache history who came in with the worst headache of her life. You gave her a cocktail that temporarily masked the symptoms. She’s back the next day because the headache never actually went away, and now she can’t see right. That is not a migraine getting better. That is something getting worse.
Dr. Hayward gave her the same cocktail again. He added steroids and a triptan, but he ordered zero new imaging. No MRI. No further workup. He wrote in the chart that her symptoms improved after the medications and he discharged her with a diagnosis of migraine and vertigo.
We deposed Dr. Hayward. We asked him why he didn’t order an MRI the second time around, given that the first cocktail had only worked temporarily. He admitted the MRI was available. He admitted it could show bleeding or a clot. His answer for why he didn’t order it was that “her symptoms are all improved with the medications.”
Her symptoms weren’t improved. They were sedated. There’s a difference, and it’s the difference that killed her.
As Sarah was leaving the hospital that night, Linda watched her stumble down the hallway like she was drunk. When Linda told her to sit on a bench, Sarah dropped to the floor. A nurse had to come back and help her up.
The Third Visit to the Emergency Room
The next morning Sarah tried to take a shower and couldn’t do it. Matt drove her back to the ER. She called Linda from the car and said she didn’t know what was happening to her.
She got to the ER around 9:30 a.m. The triage nurse wrote down the chief complaint as “altered mental status.” On top of everything else, Sarah was now having trouble thinking clearly and putting words together. This was day three.
A different doctor saw her this time. He ordered a CT scan and called a neurologist. The neurologist recommended an MRI and a lumbar puncture. But before the MRI could happen, Sarah seized. Tonic-clonic. Decorticate posturing. They intubated her.
The emergency CT venogram showed it. Near-complete thrombosis of the superior sagittal sinus. A massive clot had been choking off the blood drainage from her brain, probably for days. The pressure had built until her brain started bleeding. They transferred her to another hospital for neurosurgery. The surgical team got in there, looked at the imaging, and saw there was no cerebral perfusion left. Nothing to save. Sarah was pronounced dead at 11:37 that night.
She had been married for 31 days.
What Killed Her, and How It Could Have Been Found
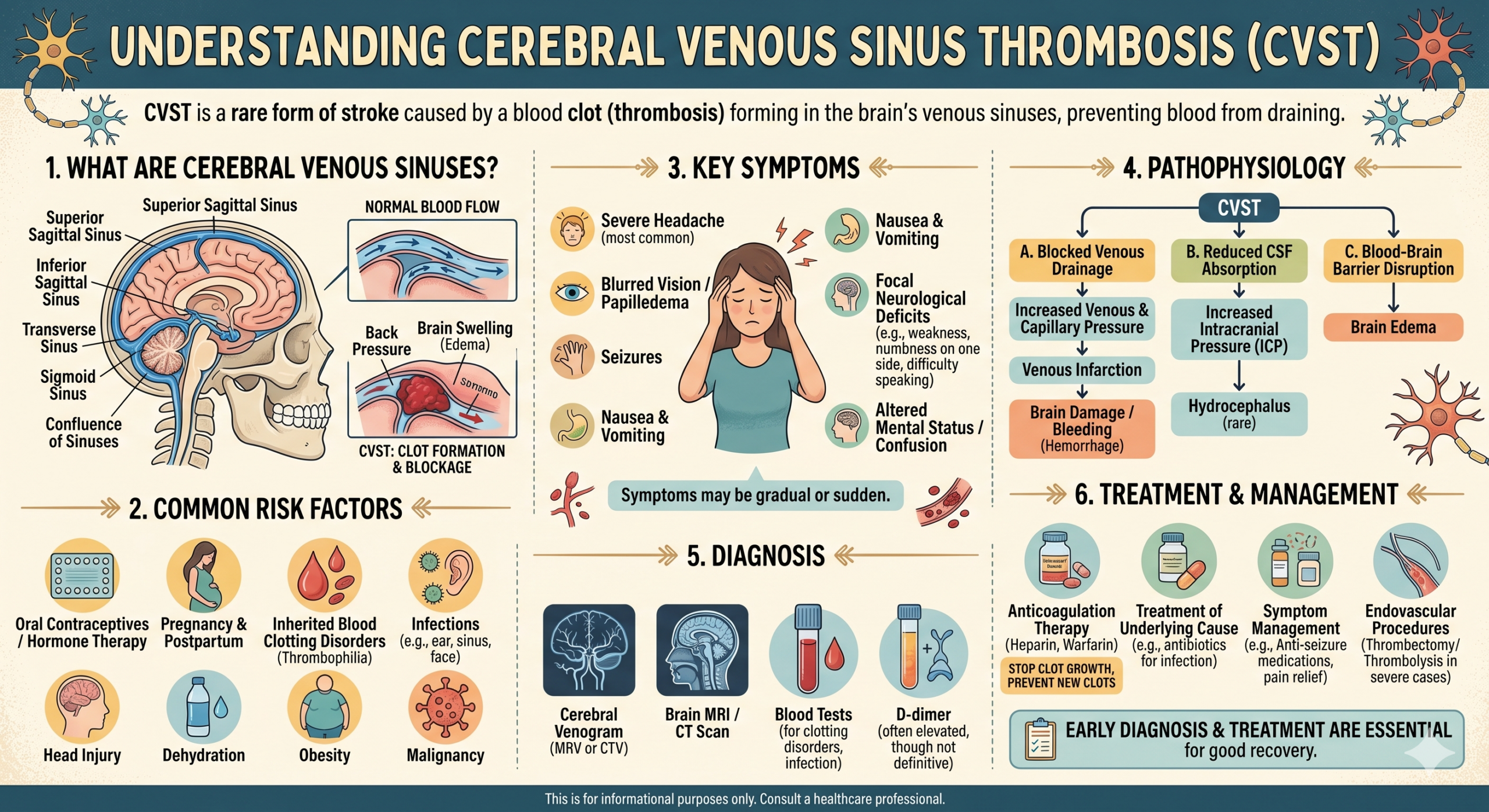
Cerebral venous sinus thrombosis. CVST. The venous sinuses are channels in the brain that drain blood back toward the heart. When a clot blocks those channels, blood has nowhere to go. Pressure builds inside the skull. Eventually the brain bleeds. If you catch it in time, you can treat it with blood thinners, monitoring in an ICU, and in some cases a procedure to physically remove the clot. If you don’t catch it, the patient dies.
CVST is rare. But it is not invisible. A CT with contrast can show it. A CT venogram can show it. An MRI can show it. And Sarah was practically waving a sign that said “look harder.” She was a young woman with zero headache history presenting with a sudden, severe, unrelenting headache that got worse over two days and added new neurological symptoms at each visit. Her bloodwork showed a low platelet count, which can signal an active clotting process. She’d had the J&J COVID vaccine two weeks prior, a vaccine that had been publicly linked to rare but serious blood clotting events. The urgent care PA spotted the red flags in minutes. Dr. Hayward missed them over two days and three visits.
The Standard of Care
Emergency medicine has a concept called the “first or worst” headache rule. When a patient shows up with a headache they describe as the first or worst of their life, you don’t just treat the pain and send them home. You work it up. You image the brain. You rule out the dangerous stuff, because the dangerous stuff kills people.
That obligation only increases when the patient comes back. A return visit for the same complaint, with new or worsening symptoms, is a clear signal that your initial diagnosis was wrong or incomplete. The standard of care at that point requires you to broaden your differential diagnosis and order additional testing. Giving the same cocktail a second time and hoping for a different result is not medicine. It is wishful thinking.
Our emergency medicine expert, a professor at a leading academic medical center, opined that Dr. Hayward fell below the standard of care on both visits. Our neuroradiology expert confirmed that any of several imaging studies would have, more likely than not, revealed the clot. If it had been found, Sarah would have been admitted to an ICU, started on appropriate anticoagulation therapy, and given access to interventional procedures. She would have had a chance.
What the Defense Argued
The defense brought in their own ER doctor from a major academic institution. He said the care was fine. Headaches are common. CVST is vanishingly rare. The patient responded to treatment. The migraine diagnosis was reasonable.
They also hired a neurologist who argued that even if the clot had been found earlier, the particular type of clotting disorder Sarah had was so aggressive that she would have died regardless. Inevitable death, they called it. No treatment at any point would have changed anything.
We took those arguments apart piece by piece. On standard of care, we had something powerful that no defense expert could explain away. A physician assistant at an urgent care clinic recognized the danger after a single visit and immediately referred Sarah for hospital-level imaging. Dr. Hayward saw her twice, over two days, with escalating symptoms, and never ordered that imaging. If the standard of care didn’t require it, why did the PA think it did? On causation, our experts testified that earlier diagnosis and treatment would have given Sarah a meaningful chance at survival. The medical literature on CVST does not support the claim that every case is inevitably fatal. People survive this. But only if someone finds it.
The case settled for $2.1 million before trial.
What This Case Was About
You can’t give a family their daughter back. You can’t undo a wedding that became a memorial. No verdict and no settlement makes that right.
But you can make sure that the people responsible are held accountable. You can make sure that a hospital and a doctor answer for the decision to treat a dying woman’s symptoms three times without ever investigating the cause. And you can send a message to every emergency department that this is not an acceptable way to practice medicine.
That is what this case was about.
This case study is based on an actual matter handled by Lupetin & Unatin, LLC. Names and identifying details have been changed to protect the confidentiality of the settlement and the privacy of the parties involved. The settlement amount reflects the resolution of this particular case and is not a guarantee of results in any other matter.