Delayed Diagnosis of Colorectal Cancer
If you or someone you love was diagnosed with colon cancer at an advanced stage — and you are asking whether it should have been caught sooner — you are asking exactly the right question.
Free Consultation — No Fee Unless We Win
Lupetin & Unatin, LLC represents Pennsylvania patients who experienced a delay in diagnosis due to medical negligence by doctors or other medical professionals.
Delayed diagnosis of colorectal cancer is not always an unavoidable tragedy. In many cases it is the direct result of a physician’s failure to screen appropriately, to recognize the warning signs, to follow up an abnormal test result, or to refer a patient for specialist evaluation. At Lupetin & Unatin, we investigate these cases, and we know how to determine whether your right to reasonable medical care was violated.
At A Glance
The Problem
My doctor missed my colon cancer. My symptoms were dismissed for months. I was diagnosed at Stage III or Stage IV — could it have been caught sooner?
If you are asking those questions, you are in the right place. A delayed or missed diagnosis of colorectal cancer is not always an unavoidable outcome. In many cases it is a preventable medical failure: a physician who did not order a colonoscopy when the guidelines required one, did not follow up a positive stool test, or dismissed rectal bleeding and anemia as benign without ruling out malignancy. The difference between a Stage I diagnosis — where roughly nine in ten patients survive five years — and a Stage IV diagnosis — where fewer than one in seven do — is the difference that a timely diagnosis makes. When a physician’s failure closes that window, Pennsylvania law may provide a remedy.
Most Common Medical Errors in Colon Cancer Cases
The symptom most often dismissed is rectal bleeding — routinely and wrongly attributed to hemorrhoids by primary care physicians who do not perform a digital rectal exam or order further workup, particularly in patients who have risk factors or are over age 45. Iron-deficiency anemia in an adult male or postmenopausal woman — which should prompt immediate colonoscopy under AGA guidelines — is frequently managed with iron supplements while the underlying source of blood loss goes uninvestigated. The screening failure seen most often is the positive stool-based test (FIT or Cologuard) that generates an abnormal result in the electronic health record but is never communicated to the patient and never followed by the colonoscopy that guidelines require. Gastroenterologists contribute to delay when they perform an incomplete colonoscopy — failing to visualize the full colon — and then tell the patient everything looked normal without scheduling appropriate follow-up imaging. Radiologists and pathologists complete the picture: a CT report that calls colonic wall thickening “nonspecific” without recommending colonoscopy, or a polyp specimen signed out without adequate staging, can each be an independent act of negligence.
How Lupetin & Unatin Can Help
At Lupetin & Unatin, we investigate colon cancer misdiagnosis cases throughout Pennsylvania — pulling every relevant record, from colonoscopy reports and pathology specimens to primary care charts and radiology reads, to determine precisely where and why the diagnosis was delayed. When you call, you speak with an attorney, not a paralegal. The case review is free, and we handle these matters on a contingency fee basis: no fee of any kind unless we recover compensation for you.
What Is Colon Cancer and Why Does Early Diagnosis Matter?
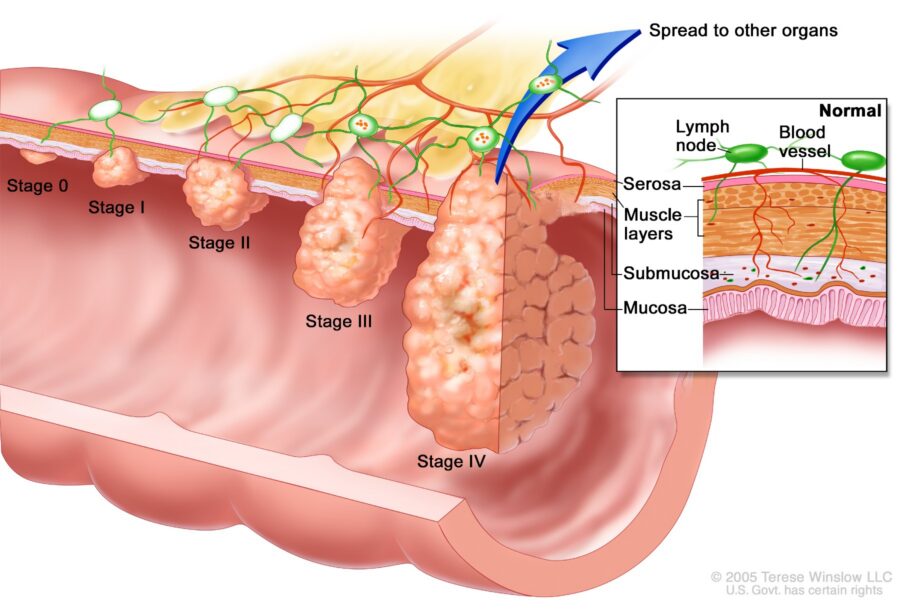
Colorectal cancer arises from the inner lining of the large intestine — most commonly from small growths called polyps that develop over years and can transform into malignant tumors if left in place. The term ‘colorectal cancer’ encompasses cancers of the colon (the main body of the large intestine) and the rectum (its terminal segment), which together are treated as a single disease category for most diagnostic and screening purposes.
The great majority of colorectal cancers — roughly 95 percent — are adenocarcinomas, meaning they originate in the glandular cells that line the colon wall. Less common subtypes include mucinous carcinomas, signet ring cell carcinomas, and carcinoid tumors, each of which has its own prognostic implications. Hereditary syndromes including Lynch syndrome (hereditary nonpolyposis colorectal cancer, or HNPCC) and familial adenomatous polyposis (FAP) account for a meaningful portion of cases in younger patients and impose specific screening obligations on treating physicians.
According to the American Cancer Society, colorectal cancer is the third most common cancer diagnosed in both men and women in the United States, and the second leading cause of cancer-related death when men and women are combined. The National Cancer Institute’s Surveillance, Epidemiology, and End Results (NCI SEER) program tracks five-year relative survival rates by stage, and those numbers tell the central story of why early diagnosis is critical. The table below summarizes what a patient’s prognosis looks like depending on the stage at which the cancer is found.
| Stage | Description | 5-Year Relative Survival Rate (ACS / NCI SEER) |
|---|---|---|
| Stage I | Cancer confined to inner layers of colon wall | ~90% |
| Stage II | Cancer has grown through colon wall, not yet reached lymph nodes | 75-85% |
| Stage III | Cancer has spread to nearby lymph nodes | 40–70% (varies by sub-stage) |
| Stage IV | Distant metastasis (liver, lungs, peritoneum) | 16% |
Source: American Cancer Society (ACS) / National Cancer Institute SEER Program.
The difference between a Stage I diagnosis — where roughly nine in ten patients are alive five years later – and a Stage IV diagnosis – where fewer than one in seven survive to that mark – is the difference between a disease that is treated and a disease that kills.
Colorectal cancer spreads by local invasion through the bowel wall, by migration through lymphatic channels to regional lymph nodes (the pathway that moves a cancer from Stage II to Stage III), and by spreading through the bloodstream to distant organs, most commonly the liver, lungs, and peritoneum. Each of these pathways takes time. The window during which a cancer can be caught before it crosses from curable to incurable is real, and it can be closed by a physician who fails to act when a careful physician should.
Who Is Most at Risk? Risk Factors and Demographics
Colorectal cancer does not strike randomly. It follows patterns that physicians are trained to recognize and are expected to act upon. Age is the most significant single risk factor: the incidence of colon cancer rises sharply after age 45, and most cases are diagnosed in adults over 50. The United States Preventive Services Task Force (USPSTF) and the American Cancer Society have both set the recommended start age for routine screening at 45 for average-risk adults, a threshold that reflects the epidemiology of the disease. Black Americans develop colorectal cancer at higher rates and at younger ages than white Americans, and also face higher mortality — a disparity that makes age-appropriate and race-aware screening even more urgent for this population.
Family history is a critical risk amplifier. A patient with one first-degree relative diagnosed with colorectal cancer or an advanced adenoma has roughly double the average risk. The risk is higher still when the affected relative was diagnosed before age 50, or when multiple first-degree relatives are affected. Patients with known Lynch syndrome — an inherited mismatch repair gene mutation — face a lifetime risk of colorectal cancer that can exceed 50 percent. Patients with FAP have a near-certain lifetime risk if untreated.
Lifestyle and comorbid conditions also matter. Obesity, physical inactivity, heavy alcohol use, cigarette smoking, and a diet high in red and processed meats are all established risk factors, supported by decades of prospective epidemiological data. Patients with inflammatory bowel disease — Crohn’s disease and ulcerative colitis in particular — face elevated colorectal cancer risk that requires heightened surveillance, with colonoscopy intervals that differ from the general population guidelines.
Clinical Red Flags: Symptoms Physicians Must Not Dismiss
Colorectal cancer produces symptoms. Some appear early; others arise only as the disease progresses. In either case, a reasonably trained physician must recognize the clinical significance of what the patient is reporting and respond with appropriate and timely medical evaluation.
Rectal bleeding or blood in the stool.
Hematochezia — bright red blood passed with or separately from stool — is never normal in an adult and is never safely attributed to hemorrhoids without first ruling out a more serious cause in patients with risk factors or who are above average risk age. Melena (dark, tarry stools suggesting upper or lower GI blood loss) likewise demands investigation. The appropriate clinical response is a digital rectal examination, referral for colonoscopy, or at minimum a fecal occult blood test. The negligent response is to tell the patient they probably have hemorrhoids and to advise them to return if it does not resolve.
Unexplained iron-deficiency anemia.
Iron-deficiency anemia in an adult male at any age, or in a postmenopausal woman, has no dietary explanation and must be presumed to represent occult blood loss from the gastrointestinal tract until proven otherwise. The American Gastroenterological Association (AGA) and the American College of Gastroenterology (ACG) recommend colonoscopy for adults with new iron-deficiency anemia. A physician who prescribes iron supplements without investigating the source has provided inadequate care.
Change in bowel habits.
Persistent changes in stool caliber (pencil-thin stools), new-onset constipation or diarrhea lasting more than four to six weeks, or a sensation of incomplete bowel emptying (tenesmus) are all recognized warning signs. These symptoms can indicate a mass causing partial obstruction or mucosal irritation. The appropriate response is a thorough history, abdominal examination, and referral for colonoscopy, particularly in patients over 45 or those with risk factors. Attributing these symptoms to irritable bowel syndrome without ruling out malignancy may be negligent when the clinical picture does not fit and the risk profile demands further investigation.
Unintentional weight loss.
Weight loss of more than five percent of body weight over six to twelve months without an identified cause is a symptom that should prompt a systemic workup, including evaluation of the gastrointestinal tract. Combined with any of the above symptoms, unexplained weight loss in a patient of appropriate age or risk profile requires colonoscopy, not watchful waiting.
Abdominal pain or a palpable abdominal mass.
A mass palpated in the right lower quadrant or elsewhere in the abdomen is a finding that cannot be deferred. Persistent cramping or abdominal pain localized to the right or lower abdomen, particularly in the absence of another identified cause, warrants imaging and/or colonoscopy. A physician who does not document abdominal examination findings — or who performs none — in a patient with these complaints has failed the standard of care.
The Standard of Care: Clinical Guidelines Physicians Must Follow
In Pennsylvania and across the United States, the standard of care for colorectal cancer screening, diagnosis, and workup is defined by evidence-based guidelines issued by national medical organizations. These are not aspirational targets; they represent the minimum that a competent physician in the relevant specialty is expected to know and to practice.
The USPSTF, an independent panel of primary care physicians and prevention experts appointed by the Department of Health and Human Services, recommends that all adults at average risk begin colorectal cancer screening at age 45 and continue through age 75. Acceptable screening modalities include annual high-sensitivity guaiac fecal occult blood testing (gFOBT) or fecal immunochemical testing (FIT), multi-target stool DNA testing (Cologuard) every one to three years, CT colonography every five years, or colonoscopy every ten years. The USPSTF’s 2021 recommendation statement carries a Grade B recommendation for the 45–75 age group, meaning the evidence of benefit is substantial. A primary care physician who fails to offer or document any colorectal cancer screening discussion with an eligible patient has deviated from this standard.
The American Cancer Society similarly recommends screening starting at age 45 for average-risk adults and earlier for high-risk individuals. The American College of Gastroenterology (ACG) and the American Gastroenterological Association (AGA) provide detailed colonoscopy guidelines and specify surveillance intervals after polyp removal based on polyp size, number, and histology. Patients with tubular adenomas measuring 10mm or larger, or those with three or more adenomas, require a colonoscopy follow-up in three years — not ten. A gastroenterologist who schedules a routine ten-year interval after finding a high-risk polyp has failed to comply with ACG/AGA surveillance guidelines.
For patients with a first-degree family history of colorectal cancer or an advanced polyp, the ACG recommends beginning colonoscopy screening at age 40 — or ten years before the age at which the youngest affected relative was diagnosed, whichever comes first — and repeating every five years. A physician who fails to elicit, document, and act upon a family history of colorectal cancer has allowed a modifiable risk factor to go unaddressed.
Critically, a positive stool-based screening test — whether FIT, gFOBT, or stool DNA — is not a diagnosis of cancer, but it is a mandatory gateway to colonoscopy. The ACG and AGA are unambiguous: a positive stool-based test must be followed by colonoscopy, not by repeat stool testing. Any physician or practice that receives a positive stool test result and fails to refer the patient for colonoscopy within a reasonable timeframe — generally one to three months — has breached the standard of care. And any system that generates a positive result that is never communicated to the patient has failed at the most basic level of medical practice.
Common Mechanisms of Negligent Delay: Scenarios
Scenario 1: The Dismissed Symptom in Primary Care
A 49-year-old Black man visits his family physician with a complaint of intermittent rectal bleeding over the past two months. He mentions that his father had colon cancer at age 58. His physician attributes the bleeding to internal hemorrhoids, performs no digital rectal exam, and advises the patient to use over-the-counter hemorrhoid cream and return in six weeks if the bleeding continues. The patient returns four months later when the bleeding worsens; a colonoscopy finally reveals a Stage III sigmoid adenocarcinoma. At Stage I, the tumor would have been entirely resectable. The physician’s failure to perform a rectal exam, order a colonoscopy, or refer to gastroenterology given the patient’s age, race, symptoms, and family history was a departure from the standard of care that cost this man his chance at cure.
Scenario 2: The Positive FIT Result That Went Nowhere
A 54-year-old woman completes an annual fecal immunochemical test (FIT) mailed to her by her primary care practice’s preventive health program. The test returns positive. The result is uploaded to the electronic health record, flagged as abnormal — and never communicated to the patient. Eight months later, the patient schedules a routine physical and is told, for the first time, that her FIT had been positive. By then, she has developed new symptoms of abdominal pain and fatigue; colonoscopy reveals Stage III right-sided colon cancer with regional lymph node involvement. Both the physician and the practice are potentially liable: the physician for failure to review and act on the result, and the practice under a corporate negligence theory for failing to maintain a system ensuring abnormal results are communicated.
Scenario 3: The Radiologist Who Called It ‘Nonspecific’
A 61-year-old man undergoes a CT scan of the abdomen and pelvis for unrelated flank pain. The radiologist’s report notes ‘mural thickening of the ascending colon, nonspecific, consider follow-up imaging in six months.’ The referring emergency department physician reads only the negative findings relevant to the patient’s chief complaint and discharges the patient without communicating the incidental colonic finding. No follow-up imaging is scheduled; no colonoscopy is recommended. Sixteen months later, the patient is diagnosed with Stage IV right colon cancer with liver metastases. A competent radiologist would have recommended colonoscopy, not follow-up CT, for this finding. A competent emergency physician would have communicated the incidental finding to the patient’s primary care physician.
Scenario 4: The Gastroenterologist Who Did Not Complete the Colonoscopy
A 57-year-old woman undergoes a colonoscopy during which the gastroenterologist reaches the cecum but notes poor bowel preparation in the right colon, precluding adequate visualization of that segment. The procedure note documents ‘incomplete visualization of right colon due to poor prep’ — but the patient is told only that her colonoscopy was ‘normal’ and that she does not need another one for ten years. No repeat colonoscopy is recommended; no alternative imaging is ordered. Three years later, she is diagnosed with a large right-sided colon cancer — the very region that was not adequately examined. Failure to communicate the limitations of an incomplete study and to arrange appropriate follow-up is a well-recognized mechanism of diagnostic negligence.
Scenario 5: The Pathologist Who Missed a Malignancy
A 63-year-old man undergoes colonoscopy, during which his gastroenterologist removes several polyps including one large, sessile lesion in the sigmoid colon. The pathology report characterizes the specimen as ‘tubulovillous adenoma with high-grade dysplasia’ — a finding that requires close surveillance and possible surgical consultation. The gastroenterologist, reviewing the report quickly, schedules a routine three-year follow-up without discussing the significance of high-grade dysplasia with the patient. Two years later, the patient is diagnosed with invasive adenocarcinoma at the same site, now with lymph node involvement. Whether the original pathology reading underestimated an existing carcinoma, or whether the follow-up interval was inadequate, both the pathologist and the treating gastroenterologist may share liability for the delayed diagnosis.
Standard of Care vs. Negligence — A Clinical Comparison
The table below compares the required standard of care with specific examples of negligent conduct in the diagnosis and management of colorectal cancer.
| Clinical Area | Appropriate Standard of Care | Evidence of Negligence |
|---|---|---|
| Symptom Evaluation | Perform thorough history and physical; order colonoscopy or CT colonography for patients with rectal bleeding, unexplained anemia, or change in bowel habits lasting more than four weeks, especially in patients 40+. | Attributing rectal bleeding to hemorrhoids without digital rectal exam or further workup; dismissing anemia as dietary without ruling out occult GI blood loss. |
| Screening Initiation | Begin colorectal cancer screening at age 45 for average-risk adults (USPSTF, ACS). Begin at age 40—or 10 years before youngest affected relative—for patients with first-degree relative with CRC or advanced polyp. | Failing to screen average-risk patients at all; not lowering the screening age for patients with documented family history. |
| Abnormal Screening Follow-Up | When FIT/FOBT is positive, colonoscopy must be performed within 1–3 months. When stool DNA test (Cologuard) is positive, prompt colonoscopy is required. | Repeating a stool-based test after a positive result instead of proceeding directly to colonoscopy; noting the result without issuing a referral. |
| Colonoscopy & Biopsy | Any visualized mass, ulcerated lesion, or suspicious polyp must be biopsied at the time of colonoscopy; any non-visualized segment must be documented, and the study may need to be repeated. | Withdrawing without biopsy when a suspicious lesion is observed; failing to note and communicate an incomplete colonoscopy. |
| Imaging Interpretation | Radiologist must report all colonic wall thickening, luminal masses, or pericolonic stranding; findings consistent with colorectal neoplasm should prompt a recommendation for colonoscopy. | Describing a colonic mass as 'nonspecific' without recommending follow-up; failing to communicate an urgent finding to the referring physician. |
| Pathology Review | Pathologist must render a diagnosis consistent with the submitted biopsy; adenocarcinoma must be staged appropriately; discordant findings must be flagged and reviewed. | Signing out an adenocarcinoma specimen without specifying grade or margins; failing to communicate a malignant diagnosis to the treating physician. |
| Specialist Referral | PCP must refer to gastroenterology when screening is indicated, when findings are abnormal, or when patient's risk profile warrants specialist evaluation. | Failing to refer a 48-year-old patient with hematochezia and family history because the patient 'didn't want a colonoscopy.' |
| Results Communication | Abnormal laboratory or imaging results must be communicated directly to the patient and documented; a follow-up plan must be established and confirmed. | Sending a letter that the patient never received; documenting a result in the chart without ensuring patient awareness or scheduling follow-up. |
What Makes a Colon Cancer Misdiagnosis Case Legally Viable?
To pursue a delayed diagnosis claim in Pennsylvania, a plaintiff must establish four elements: duty of care, breach of that duty, causation, and damages. In the context of colorectal cancer, these elements translate into concrete, case-specific inquiries.
Duty of care is established by the physician-patient relationship. If a physician saw, treated, or was responsible for a patient’s care during the period when the cancer should have been diagnosed, a duty existed.
Breach of the standard of care is established through expert testimony. Pennsylvania law requires that a plaintiff’s expert be board-certified in a relevant specialty and offer an opinion that the defendant’s conduct fell below what a reasonably trained physician in that specialty would have done in the same or similar circumstances. The scenarios described above — the missed positive FIT result, the undisclosed incomplete colonoscopy, the dismissed rectal bleeding — all represent potentially provable breaches.
Causation is where colorectal cancer cases turn on the facts of stage progression. The central argument is that the physician’s breach caused — or materially contributed to — the cancer advancing from a stage at which it was curable to a stage at which it was not. Pennsylvania courts recognize the ‘lost chance’ doctrine, which provides that a defendant is liable when negligence has substantially diminished a patient’s opportunity for a better outcome, even if the patient’s ultimate death or serious harm cannot be attributed with certainty to the delay alone. In Mitzelfelt v. Kamrin (1990), the Pennsylvania Supreme Court recognized that a patient who loses a substantial chance of survival due to a physician’s negligence has suffered a compensable harm. In colorectal cancer cases, this doctrine allows plaintiffs to recover for the difference in survival probability between the stage at which the cancer should have been caught (e.g., Stage II, with an 80% five-year survival rate) and the stage at which it actually was diagnosed (e.g., Stage IV, with a 16% five-year survival rate). That difference in probability — approximately 64 percentage points — represents a material reduction in the chance of survival.
Damages include the full spectrum of losses caused by the delay — not the cancer itself, but the worsening of the cancer’s course. We address damages in detail in the next section.
What Is a Colon Cancer Misdiagnosis Case Worth in Pennsylvania?
Pennsylvania places no statutory cap on compensatory damages in medical malpractice cases. The Pennsylvania Medical Care Availability and Reduction of Error (MCARE) Act, enacted in 2002, eliminated the prior damages cap structure, meaning that plaintiffs are entitled to full economic and non-economic compensation for their losses.
Economic damages in a delayed colorectal cancer diagnosis case include the cost of medical treatment that would not have been necessary had the cancer been caught earlier — additional chemotherapy regimens, surgical procedures, hospital admissions, and radiation therapy that a Stage I patient would not have required. They also include lost wages and diminished earning capacity for patients who can no longer work during extended treatment, and future care costs including home health services, palliative care, and end-of-life care in wrongful death cases.
Non-economic damages include the patient’s physical pain and suffering endured through advanced cancer treatment — surgeries, chemotherapy, colostomy, and the indignities of aggressive palliative care — that would not have been necessary. They include loss of life’s pleasures: the inability to work, to engage in hobbies, to parent, to be present in a spouse’s or child’s life as the disease progresses. They include loss of consortium claims by a spouse or domestic partner. In cases where the patient has died, the estate may pursue a wrongful death claim and a survival action under Pennsylvania law, both of which may be brought simultaneously.
Pennsylvania Law: Filing a Colon Cancer Malpractice Claim
Statute of Limitations
Under the PA MCARE Act, a medical malpractice claim must generally be filed within two years of the date on which the cause of action accrued. In delayed diagnosis cases, this is often the date on which the patient was actually diagnosed with cancer — since that is typically when the patient first knew, or reasonably should have known, that a medical error may have contributed to the harm. Pennsylvania’s discovery rule extends the limitations period when the patient could not, through reasonable diligence, have discovered the injury and its cause earlier. Courts apply this rule on a case-by-case basis, and it is a fact-intensive inquiry. For cases involving minor patients, the statute of limitations is tolled until the patient turns 18.
Certificate of Merit
Pennsylvania Rule of Civil Procedure 1042.3 requires that every medical malpractice plaintiff file a Certificate of Merit within 60 days of commencing the lawsuit. The certificate must be signed by a licensed physician who is board-certified or board-eligible in the same specialty as the defendant, and who has reviewed the case and determined that there is a reasonable probability that the defendant’s conduct fell below the standard of care. Filing a complaint without timely filing a certificate — or filing one signed by an unqualified expert — can result in dismissal of the case. At Lupetin & Unatin, we retain qualified expert reviewers before filing, and the Certificate of Merit requirement is met as a matter of our standard practice.
Hospital Liability
Pennsylvania recognizes both respondeat superior liability — under which a hospital is vicariously responsible for the negligent acts of its employed physicians and staff — and corporate negligence, under which a hospital can be held directly liable for systemic failures such as inadequate credentialing, deficient policies for communicating abnormal test results, or failure to maintain systems ensuring that critical findings reach treating physicians. In cases where an abnormal colonoscopy result, CT finding, or pathology report was lost in a practice’s administrative system, the corporate negligence theory may be the primary vehicle for holding the institution accountable.
Frequently Asked Questions
It does not necessarily hurt it. The relevant question is not how long the cancer was growing, but when a reasonably careful physician should have detected it given your symptoms, risk factors, and medical history — and how much worse your prognosis became because of the delay. A slow-growing cancer that should have been caught at Stage I two years before your diagnosis is just as much a malpractice case as one that progressed rapidly. Expert witnesses in these cases routinely address tumor biology and the timeline of detectable symptoms.
Yes. Pathologists are held to the same standard of care as other physicians, and a misread biopsy — one that fails to identify adenocarcinoma, or that understages the disease — can form the basis for a malpractice claim. Similarly, if a biopsy result was never communicated to the treating physician, or was communicated but never transmitted to the patient, both the pathologist and the practice or hospital may be liable. We review all pathology reports and laboratory records as part of our investigation in every colorectal cancer case.
No — and in some ways it strengthens it. If you have Lynch syndrome, FAP, or a significant family history, your physician had a legal obligation to recognize that elevated risk, to begin screening earlier than the general population average, and to conduct surveillance at shortened intervals. A physician who failed to take a family history, failed to act on a documented history, or failed to refer you to a genetic counselor when your history warranted it may have breached a heightened duty of care. Hereditary risk is not a defense for the physician; it is an additional obligation.
Not necessarily. The harm in a delayed diagnosis claim is measured by stage progression — by what spread to your lymph nodes or distant organs during the months or years the cancer went undetected. A small tumor that has already metastasized to lymph nodes is a Stage III cancer with a substantially worse prognosis than a slightly larger tumor confined to the bowel wall. Stage and lymph node involvement, not tumor size alone, determine prognosis and guide the causation analysis in your case.
Potentially, yes. Many colorectal cancers — particularly right-sided tumors — produce few or no symptoms until they are advanced. This is precisely why screening exists. If your physician failed to initiate or offer age-appropriate screening, failed to follow up after a positive stool test, or failed to recommend colonoscopy given your risk profile, the absence of dramatic symptoms does not excuse that failure. The screening guidelines exist for this reason exactly.
The general rule is two years from the date you knew or reasonably should have known that a medical error contributed to your diagnosis or its worsening. In practice, for most patients, that clock begins running when they receive their cancer diagnosis and begin to question why it was not caught earlier. We recommend contacting us as soon as possible so that we can evaluate the timing of your claim and preserve critical evidence.
No. At Lupetin & Unatin, we handle medical malpractice cases on a contingency fee basis, which means we charge no fee unless and until we recover compensation for you. The initial case review, the expert medical analysis, and all costs of investigation and litigation are advanced by the firm. You will not receive a bill from us if we take your case and do not recover.
Why Lupetin & Unatin Investigates Colon Cancer Malpractice Cases
Colorectal cancer misdiagnosis cases require more than legal skill — they require the ability to read and interpret years’ worth of medical records, to identify precisely where in the timeline of screening, testing, and follow-up a physician departed from what the guidelines required, and to engage expert witnesses who can translate complex colonoscopy reports, pathology specimens, and staging criteria into testimony a jury will understand and credit. At Lupetin & Unatin, we know how to access the board-certified expert witnesses — gastroenterologists, oncologists, colorectal surgeons, radiologists, and pathologists — who can review your records and offer the opinions that Pennsylvania law requires. We obtain and analyze every relevant document: primary care records, colonoscopy reports, pathology slides, radiology imaging and reads, laboratory results, and communications between providers. We pursue these cases because we understand that the difference between a curable cancer and a fatal one often comes down to a physician’s failure to do what the standard of care required — and because the people harmed by that failure deserve accountability.
What to Expect When You Call
When you contact Lupetin & Unatin, we will ask you to describe what happened in your own words: your symptoms, the physicians you saw, the tests you had, when your cancer was diagnosed, and what stage it was at diagnosis. We will explain, in plain terms, what we are looking for in the medical record and what the investigation process involves.
If you decide to proceed, we handle all records retrieval. We will request your complete medical records from every relevant provider and we will review those records in full before retaining an expert. Once we have the records, one or more physician experts review the case and gives us a candid assessment of merit. We will share that assessment with you honestly, even if the conclusion is that a case cannot be supported. We do not take cases we do not believe in or which an expert cannot support.
If the expert confirms a deviation from the standard of care, we will explain your legal options, the likely timeline, and how the contingency fee structure works. You will have a clear picture of what pursuing a claim involves before you decide to move forward. We do not rush that conversation. The decision is yours.
Contact Lupetin & Unatin
If you believe that your colon cancer — or a loved one’s — was diagnosed too late because a physician failed to screen, failed to follow up, or failed to recognize the warning signs that were already there, we want to hear from you. A call to our Pittsburgh office is a conversation, not a commitment. We will listen, we will be honest about what we see, and if there is a case to pursue, we will pursue it fully. Lupetin & Unatin, LLC represents patients and families throughout Pennsylvania from our office at 310 Grant Street, Grant Building, Suite 3204, Pittsburgh, PA 15219. You can reach us at 412-281-4100, or visit us at pamedmal.com.
Sources and Citations
The following guidelines, statistics, and clinical references are cited in this article.
Clinical Guidelines
- United States Preventive Services Task Force (USPSTF): Colorectal Cancer: Screening. Final Recommendation Statement, May 2021 (Current as of 2026). Grade B Recommendation for adults aged 45–75.
- American Cancer Society (ACS): Colorectal Cancer Screening Guidelines (2026 Edition). Current recommendation: begin screening at age 45 for average-risk adults.
- American College of Gastroenterology (ACG): ACG Clinical Guideline: Colorectal Cancer Screening. Rex DK et al. American Journal of Gastroenterology.
- American Gastroenterological Association (AGA): AGA Clinical Practice Guidelines on the Management of Iron Deficiency Anemia (2020/2025 Updates).
- National Comprehensive Cancer Network (NCCN): NCCN Guidelines: Colorectal Cancer Screening. Current version available at nccn.org.
Epidemiology and Survival Statistics
- National Cancer Institute: Surveillance, Epidemiology, and End Results (SEER) Program. Cancer Stat Facts: Colorectal Cancer (2026 Release). Five-year relative survival rates by stage.
- American Cancer Society: Cancer Facts & Figures 2026. Five-year relative survival rates for colorectal cancer.
- American Cancer Society: Colorectal Cancer Facts & Figures (Current Edition). Racial/ethnic disparities in CRC incidence and mortality.
Pennsylvania Law References
- Pennsylvania Medical Care Availability and Reduction of Error (MCARE) Act: 40 P.S. § 1303.101 et seq.
- Statute of Limitations: 40 P.S. § 1303.513. No cap on compensatory damages.
- Pennsylvania Rule of Civil Procedure 1042.3: Certificate of Merit requirement in professional liability actions.
- Mitzelfelt v. Kamrin, 526 Pa. 54, 584 A.2d 888 (1990). Pennsylvania Supreme Court recognition of the “lost chance” doctrine in medical malpractice.